

What is Video Capsule Endoscopy?

Video capsule endoscopy is a relatively new Outpatient procedure which enables effortless examination of the lining of the gastrointestinal tract. It is particularly suited to the small bowel which is made up of 3 parts: duodenum (top), jejunum (middle) and ileum (end). The small bowel cannot be reached and so examined by traditional gastroscopy and colonoscopy.
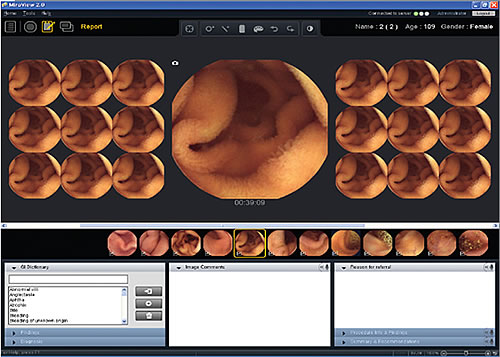
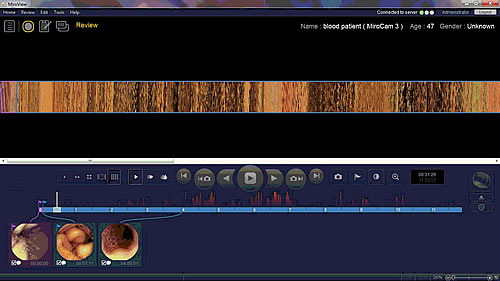
It involves swallowing a pill sized camera (with it’s own light source and battery) which then naturally travels through the gastrointestinal tract recording images. These images are wirelessly transmitted to a small receiver which you wear during the procedure. The procedure lasts approximately 8 hours (30 minutes setting up in morning and 15 minutes to finish in the evening) but you can perform your usual daily activities during the test and do not need to remain on site in hospital.
Video capsule endoscopy is a useful test in conjunction with traditional endoscopy and is usually performed when other tests are normal. It is used to investigate persistent anaemia and detect obscure gastrointestinal bleeding. It is also used to diagnose Crohn’s and Coeliac disease and evaluate prolonged cases of diarrhoea. It can also be used to detect small bowel ulceration and can offer crude information about gastric, small bowel and colonic gut transit times.

Indications for Video Capsule Endoscopy
A capsule endoscopy might be recommended to investigate the following symptoms:
- Unexplained anaemia (low blood levels)
- Unexplained abdominal pain
- Unexplained nausea and vomiting
- Unexplained weight loss
- Unexplained persistent diarrhoea
- Unexplained blood in your stools (obscure bleeding)
- To check for inflammation/ulcers
- To check/assess for inflammatory bowel disease/Crohn’s disease
- To check for coeliac disease
- To check gut transit times
Alternatives to Video Capsule Endoscopy
Capsule endoscopy is an extremely safe and easy test to perform. It is the gold standard for examining the small bowel. Endoscopy of the small bowel (small bowel enteroscopy) can be performed but is invasive, technically challenging, requires strict bowel preparation and has a poor success rate. MRI small bowel enteroscopy is a non-invasive scan but it is not as accurate as capsule endoscopy for detecting small or subtle abnormalities. Abdominal CT can also be performed but is not as accurate as MRI and involves a small dose of radiation. However, there are cases where capsule endoscopy is not the most suitable test and MRI or CT may be more appropriate.
Preparing for Video Capsule Endoscopy
Please ensure you tell Dr Goel and the endoscopy team before the day of the procedure if you:
- Have any swallowing problems
- Have had any abdominal surgery
- Have a previous history of small bowel obstruction
- Are diabetic
- May be pregnant
- Have a cardiac pacemaker
- Have a implantable cardiac defbrillator
It is important that the stomach and small bowel are empty to enable an optimal examination and allow the small bowel lining to be viewed clearly. Therefore, you should avoid eating or drinking anything for at least 6 hours before the procedure. This is usually achieved by an overnight fast as the procedure is usually carried out in the morning. Do not take any medications for at least two hours prior to the examination.
On the day of the procedure, do not apply any lotions to your abdomen. You should wear comfortable and loose two piece clothing. One piece clothing should not be worn as a sensor belt will be attached around the abdomen.
Medication Advice
Most usual medications can be continued up till the night before the procedure, however, specific precautions may be taken in some cases. If taking constipating agents such as iron tablets, loperamide (Imodium), codeine phosphate, etc., these should be stopped 1 week prior to examination. Blood-thinning drugs (e.g. Clopidogrel, warfarin, apixaban) can be continued. Please discuss any questions with Dr Goel or your nurse beforehand so appropriate advice can be given. Please also mention any allergies you may have in advance of your test.
The Video Capsule Endoscopy Procedure
Upon your arrival, you will be greeted by a member of staff who will help you prepare for your procedure. Your nurse will ask you a few pre-assessment questions and you should inform them of your medications, allergies and any potential concerns. You can ask any questions to ensure you understand the procedure. If not already done beforehand, you will be asked to sign a consent form.
Your nurse will ask you to remove your raise your upper garments and will gently attach a discreet sensor belt around your abdomen just above your waist. This is connected to a small data recorder and receiver (about the size of a mobile phone) on the belt. The sensor belt is comfortable and usually not visible beneath your clothes.
You will be given a small drink containing a ‘bubble break’ solution which helps to improve examination views. You will then be asked to swallow the pill sized video capsule and the examination will begin. You can then leave department and go home or carry out your daily activities. You may only drink water for the first 4 hours following swallowing the capsule, however, after this you can eat and drink as normal including taking any medications.
You will be asked to return to the department in the evening (usually around 8 hours) and the equipment and receiver will be taken from you. The examination video images are then downloaded to a computer and sent to Dr Goel who will then read them and write a report.
The capsule is passed naturally in the stool when you go to the toilet. However, if you begin to experience severe pain or nausea and vomiting after being discharged, you should see an emergency doctor right away.
Sedation and Anaesthesia
Video capsule endoscopy is completely painless and does not require any form of sedation or pain relief.
Risks of Video Capsule Endoscopy
Video capsule endoscopy is incredibly safe and complications are very rare. The main complication rate is of capsule retention (the capsule getting stuck) and this occurs in less than 1 in 100 cases. If capsule retention does occur, this usually resolves by itself and the capsule eventually passes through, however, rarely surgery may be required. This is performed to remove the capsule but also the cause of retention (e.g. An abnormal narrowing) and so also diagnoses and treats the cause of the abnormality. You must not undergo any form of MRI investigations whilst the capsule is in your bowel as this can be very dangerous. The video capsule examinations are read very carefully and thoroughly, however, rarely, tiny abnormalities may be missed. Dr Goel will always ensure the test is safe and appropriate for you. Any risks of the procedure will be discussed with you and you will be fully informed beforehand.